
Orthotic helmet therapy in the treatment of plagiocephaly

Jack. Orthomerica Starband
Orthotic (helmet) therapy in the treatment of plagiocephaly, Goh JL, Bauer DF, Durham SR, Stotland MA. Neurosurg Focus. 2013 Oct;35(4):E2. doi: 10.3171/2013.7.FOCUS13260. Review.
| Abstract |
| Object |
The goal of this study was to review the current literature on orthotic (helmet) therapy use in the treatment of deformational plagiocephaly.
| Methods |
PubMed was used to search English articles using the medical subject headings “deformational plagiocephaly” and “orthosis,” and “deformational plagiocephaly” and “helmet.”
| Results |
Forty-two articles were found. There were no Class I studies, 7 Class II studies, 1 Class III study, and 13 Class IV studies. Cranial orthoses have been shown to be effective in treating deformational plagiocephaly. It continues to be debated as to whether the statistical significance of treatment with cranial orthoses compared with conservative therapies is clinically significant.
Children older than 12 months of age with deformational plagiocephaly may still benefit from orthotic therapy. The long-term effects of orthotic therapy are controversial.
| Conclusions |
There is a lack of Class I literature evidence supporting the use of helmet therapy in deformational plagiocephaly. There are controversies surrounding the use of orthotic therapy such as appropriate use, cost, use in older children, and long-term outcomes. Clinical indications for orthotic therapy need to be better defined with further research studies.
In 1992, the American Academy of Pediatrics Task Force recommended that infants be placed on their backs during sleep to reduce the risk of sudden infant death syndrome. Following this “Back to Sleep” recommendation, a significant drop in sudden infant death syndrome and an associated increase in the incidence of deformational plagiocephaly was noted, and the use of cranial orthoses have been commonplace for the treatment of deformational plagiocephaly.
| Brief history of orthotic therapy |
A cranial orthotic device is also referred to as a cranial helmet, cranial orthosis, or cranial band. These devices were first described in the scientific literature by Clarren et al. in 1979. However, the idea of using artificial cranial deformation was conceived at least 30,000 years ago in ancient Peru, where infant skulls were artificially shaped using external compression with fixed boards and pads or ritual head wrapping.
Modern-day cranial orthotic devices use that same principle. They are usually custom fit and molded to allow for growth in certain regions of the cranium and concomitant growth restriction in others. Most helmets apply passive restriction rather than active compression forces, encouraging the infant’s malleable and rapidly expanding skull to grow into a desired configuration.
There are helmets that reportedly apply active molding forces to aid in the corrections, such as the Dynamic Orthotic Cranioplasty Band (Cranial Technologics, Inc.) and the pneumatic orthotic helmet described by Lee et al. Some researchers argue that there is no true distinction between passive and active devices because the application of constant active pressure would easily exceed the ischemic tolerance of the overlying skin and lead to pressure ulceration.
In the US, many cranial orthotic devices have been FDA regulated. There were currently 37 FDA-approved cranial orthoses listed on the FDA website .
| ☞ See Table 1. Devices in the original 2013 report. ☞ See Table 1a. A search on May 27, 2019 yielded 10 cranial orthoses. |
Of note, there has been some controversy surrounding the regulation of cranial orthoses. Many argue that FDA regulation helped standardize the industry, while others argue that it has caused an increase in treatment-associated costs due to centralized production of the orthoses by larger companies.
☞ TABLE 1: List of FDA-approved cranial orthotic devices. FDA 510(K) Premarket Notification. JL Goh et al. 2013. Page 2.
| Device Name | Applicant | 510(K) Number | Decision Date |
| Cranial Molding Orthosis |
ORTHOTIC SOLUTIONS, INC. |
K010273 | 04/25/2001 |
| Starband Cranial Orthosis |
ORTHOMERICA PRODUCTS, INC. |
K011350 | 07/03/2001 |
| Lerman & Son Cranial Orthosis Helmet |
LERMAN & SON | K012830 | 11/20/2001 |
| Becker Band Cranial Remolding Orthosis |
BECKER ORTHOPEDIC APPLIANCE CO. |
K013719 | 02/05/2002 |
| Static Cranioplasty Orthosis |
EASTERN CRANIAL AFFILIATES |
K020448 | 04/12/2002 |
| Cranial Solution Orthosis |
CRANIAL SOLUTIONS | K063133 | 07/02/2007 |
| Boston-Band Cranial Remodling Orthosis |
BOSTON BRACE INTL., INC. |
K072862 | 01/22/2008 |
| Camlab Cranial Orthosis Helmet |
BIOSCULPTOR CORPORATION |
K081787 | 01/27/2009 |
| Michigan Cranial Reshaping Orthosis |
DANMAR PRODUCTS, INC. |
K090341 | 01/06/2010 |
| Cranial Remolding Orthosis |
ORTHOTIC CARE SERVICES, LLP |
K111247 | 08/15/2011 |
| ☞ TABLE 1a: List of FDA cleared cranial orthotic devices. This search performed May 27, 2019 yielded 10 cranial orthoses. FDA 510(K) Premarket Notification. | |||
| Methods of anthropometric assessment |
Cranial measurements have traditionally been obtained using anthropometric calipers. Recent technological advances such as photogrammetry or 3D surface scanning with a laser allow clinicians and researchers to use more accurate and efficient measurement. The common anthropometric measurements used are explained in Table 2.

Figure 3. 3D measurement plane, sagittal plane, and coronal plane, dividing the cranium into four quadrants. ACAI =ratio of the anterior cuboid volumes and PCAI =ratio of the posterior cuboid volumes using the formula: (larger cuboid volume − smaller cuboid volume) / smaller cuboid volume × 100%. Aarnivala, Vuollo et al.
| Current research on helmet therapy |
The rise in prevalence of deformational plagiocephaly secondary to the “Back to Sleep” campaign has fueled a significant amount of research regarding the use of cranial orthotic devices as a means of correcting infantile cranial deformity. This paper focuses on the role of orthotic therapy in treating deformational plagiocephaly.
| Methods |
PubMed was used to search English articles with the following medical subject heading terms “deformational plagiocephaly” and “orthosis,” and “deformational plagiocephaly” and “helmet.”
To judge the quality of the studies, the following classifications were used:
| Class I | Evidence from a randomized controlled trial |
| Class II | Evidence from a prospective trial that compared more than 2 treatments in a non-randomized manner |
| Class III | Evidence from a prospective or retrospective case series with historical controls |
| Class IV | Evidence from a prospective or retrospective case series with no control or comparison group |
| Results |
Forty-two articles were found using the search terms detailed above. Six articles were excluded because they were not directly related to cranial orthoses therapy in deformational plagiocephaly (n = 5), or involved nonhuman subjects (n = 1).
Of the remaining 36 papers,
- 21 were primary research literature articles,
- 12 were reviews,
- 2 were letters, and
- 1 described the methodology of an ongoing randomized controlled trial.
Of the 21 primary research articles, there were
- 7 Class II studies,
- 1 Class III study, and
- 13 Class IV studies.
| Discussion |
This review article focuses on the controversies that exist in the use of orthotic therapy in deformational plagiocephaly.
| Helmet therapy in comparison with conservative treatments |
There is a lack of Class I evidence surrounding the use of helmet therapy in deformational plagiocephaly, as has been noted in previous review articles. Nevertheless, the general consensus is that cranial orthoses are indeed as efficacious, if not more efficacious, in treating deformational plagiocephaly as compared with other more conservative treatments.
Studies of helmet therapy often target patients who have already undergone unsuccessful osteopathy and/or physiotherapy as conservative measures. This experience consequently introduces a selection bias whereby patients who have more severe deformational plagiocephaly are selected to take part in orthotic trials. It is uncertain whether orthotic therapy is warranted to treat infants with mild to moderate deformational plagiocephaly.
Moss prescribed only neck-stretching exercises, positioning changes, and parental training to 66 infants with deformational plagiocephaly of mild to moderate severity, and found that the outcomes were comparable to infants who were treated by headbands in a previous study. However, because the rate of correction is faster if infants start using the helmets earlier, parents and providers alike may feel the pressure to begin infants with mild to moderate cases of deformational plagiocephaly on helmet therapy to prevent long-term cosmetic issues.
The actual clinical significance of a change of a few millimeters when using orthotic therapy compared with repositioning therapy is also another issue of contention. For example, Graham et al. compared repositioning with orthotic therapy and showed that orthotic therapy resulted in a 61% decrease in the reduction of diagonal difference compared with 52% in the repositioning group. While a difference of 9% was statistically significant, the absolute change was actually only 0.16 cm (or 1.6 mm).
Similarly, Lipira et al. showed in his 2010 prospective cohort study that orthotic helmets yielded statistically superior reduction in overall head asymmetry compared with active repositioning via a novel 3D surface scanning technique. However, this study also questioned the actual clinical significance of these statistically significant values in terms of quality of life, long-term outcomes, and parental satisfaction. Interestingly, another study that was aimed toward determining the optimal time to begin helmet therapy noted that some parents requested to withdraw prior to study aims being met, as they believed that the asymmetry was already corrected.
Two studies have attempted to address the issue of clinical significance compared with statistical significance by also incorporating measurements of parental satisfaction into their research study. Both studies showed that subjective assessments are often discordant with objective measurements. Katzel et al. measured both head asymmetry and improvement in ear position following helmet therapy. He also asked parents to subjectively rate the improvements in both head asymmetry and ear position before and after therapy. Interestingly, the parents’ perceived improvement in ear position were similar in magnitude to the changes in head shape, despite less impressive changes in actual ear offset.
The issue of ear position was made even more interesting in a study by Kluba et al. They observed that parents often noted ear shifts because they often have infants in their laps, and ear displacements were particularly apparent when observed from the vantage point of the parent from above. In their study, 40% of babies with deformational plagiocephaly without initial ear shift showed subsequent increased ear shift after being treated with cranial orthoses.
However, they found that subjective impressions of the babies’ ear positions as measured by ratings of medical doctors had a low concordance rate when compared with objective measures of ear shift.
The issue of clinical significance correlating with statistical significance is not a trivial one, as this could potentially affect the prevalence of use of cranial orthoses in deformational plagiocephaly. Ultimately, it is a cost-benefit analysis. These cranial orthotic devices cost anywhere from $1000 to $3500.
Part of the high cost is secondary to the fact that the companies that make most devices pride themselves on custom-making the orthosis for the baby. However, Thompson et al. reported positive results in 2009 while using a generic-sized soft foam helmet that was fitted to patients by applying extra foam padding. In the current atmosphere of burgeoning health care costs, this may potentially be more cost-effective for the health care system as a whole.
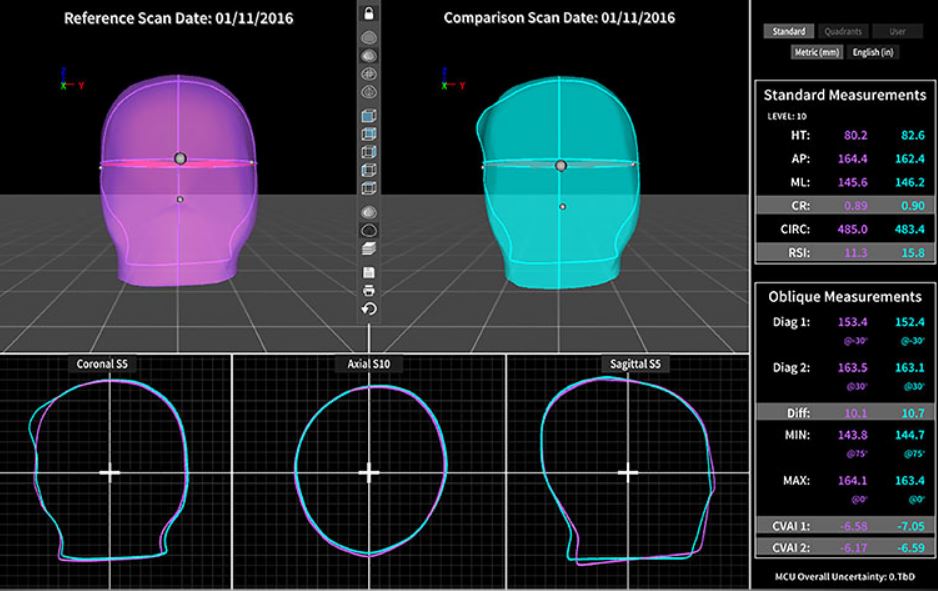
3D Measurement and Comparison Unit (MCU) software from Orthomerica allows an orthotist to provide concise and objective measurements of a child’s head shape. Whether treating conservatively, with a helmet or just monitoring for growth, the MCU will show comparative changes in growth and symmetry. OAPL Australia
| Are cranial orthoses suitable for children older than 1 year of age? |
Currently, most experts agree that starting cranial orthoses at 4 to 6 months of age is appropriate once more conservative measures have failed to correct the plagiocephaly. Kluba et al. in 2011 showed that patients who began helmet therapy prior to 6 months of age showed better relative and absolute reduction in head asymmetry when compared with patients who started after 6 months. They found that patients older than 6 months on average continued to have an abnormal cranial vault index at 4.5% at last follow-up.
This suggests that a later starting age for helmet therapy may result in incomplete resolution of the asymmetry compared with beginning helmet therapy earlier. However, there have been published case reports in which infants older than 12 months of age were treated with dynamic orthotic cranioplasty with a reduction in cranial asymmetry.
More recently, in 2013 Seruya et al. investigated the correction rate of plagiocephaly with helmet therapy in groups of infants stratified by age. They showed that the correction rate decreases with increasing infant age and that the correction rate reached the plateau rate of change (transcranial difference rate of 0.42 mm/week) once the infants were older than 32 weeks (approximately 8 months).
As such, it appears that cranial orthotic therapy continues to be warranted for older infants, but the rate of correction is slower and cranial asymmetry may not be absolutely corrected. In addition, many researchers have mentioned the logistical difficulty parents have in keeping their now more-active infant in a helmet for long periods of time per day, which may contribute toward the relatively slower rate of change documented in the literature.
| What are the long-term outcomes of deformational plagiocephaly treated with helmet therapy? |
Two studies investigating the long-term follow-up of infants treated with helmet therapy were reviewed. It appears that in terms of the cranial asymmetry itself, infants treated with helmet therapy show relatively stable anthropometric measurements after discontinuation of helmet therapy. Lee et al. showed that 5 years after helmet therapy was discontinued, very little change happened in terms of cranial vault asymmetry values and orbitotragial depth asymmetry.
Another study reviewed quality of life and parental satisfaction in long-term follow-up after treatment of plagiocephaly and found that there was no difference in quality of life between a healthy control group and infants treated with helmet therapy at 2 years after their initial clinic visit. Steinbok et al. investigated patient quality of life and parental satisfaction in school-aged children who were treated early in life with helmet therapy.
Residual asymmetry was noted by parents in 58% of respondents, with 21% expressing some concern, and only 7% of parents stating they were very concerned about the asymmetry. The children were less aware of their head asymmetry, with only 8% of children noting any asymmetry. In terms of social impact, only 5% of children reported having been teased about their head asymmetry.
| Promising future studies |
Many review papers have acknowledged the lack of randomized control trials in the deformational plagiocephaly study. However, van Wijk et al. are trying to correct this void in the literature with their current pragmatic randomized controlled trial nested in a cohort study.
Participants are recruited at 2–4 months of age when first diagnosed with deformational plagiocephaly. At 5 months of age, they will be reassessed; if the plagiocephaly persists, parents are offered the opportunity to participate in a randomized controlled trial for helmet therapy compared with conservative treatment.
Parents who decline to participate will then be part of a non-randomized controlled trial and allowed to choose helmet or non-helmet therapy. Participants will be followed at set intervals until 24 months of age. Their outcome measures will include anthropometric measures and assessments of satisfaction in parents. Final results of this trial are expected in 2013.
| Conclusions |
In this study we demonstrate a lack of Class I literature evidence supporting the use of helmet therapy in deformational plagiocephaly and address the issues of appropriate use, cost, use in older children, and long-term outcomes. Hopefully, as new research studies address these issues, the clinical indications for helmet therapy in deformational plagiocephaly will be better defined.
Source Journal of Neurosurgery, American Association of Neurological Surgeons
| References |
- An increase in infant cranial deformity with supine sleeping position, Argenta LC, David LR, Wilson JA, Bell WO. J Craniofac Surg. 1996 Jan;7(1):5-11.
- The sociopolitical history and physiological underpinnings of skull deformation, Ayer A, Campbell A, Appelboom G, Hwang BY, McDowell M, Piazza M, Feldstein NA, Anderson RC. Neurosurg Focus. 2010 Dec;29(6):E1. doi: 10.3171/2010.9.FOCUS10202.
- Head moulding for plagiocephaly, Carter MR. Arch Dis Child. 2008 Sep;93(9):809-10. doi: 10.1136/adc.2007.122309. Review. No abstract available. Full text
- Helmet treatment for plagiocephaly and congenital muscular torticollis, Clarren SK, Smith DW, Hanson JW. J Pediatr. 1979 Jan;94(1):43-6.
- Posterior positional plagiocephaly treated with cranial remodeling orthosis, de Ribaupierre S, Vernet O, Rilliet B, Cavin B, Kalina D, Leyvraz P-. Swiss Med Wkly. 2007 Jun 30;137(25-26):368-72.
- Parental satisfaction with the CranioCap: a new cranial orthosis for deformational plagiocephaly, Elwood ET, Petronio J, Wood RJ. Cleft Palate Craniofac J. 2005 Jul;42(4):340-3.
- Evidence-based care of the child with deformational plagiocephaly, part II: management, Flannery AB, Looman WS, Kemper K. J Pediatr Health Care. 2012 Sep-Oct;26(5):320-31. doi: 10.1016/j.pedhc.2011.10.002. Review.
- Plagiocephaly, brachycephaly and cranial orthotic devices: misshapen heads and helmets, Gill D, Walsh J. Arch Dis Child. 2008 Sep;93(9):805-7. doi: 10.1136/adc.2006.108746. Review. No abstract available. Full text
- Molding therapy of positional plagiocephaly: subjective outcome and quality of life, Govaert B, Michels A, Colla C, van der Hulst R. J Craniofac Surg. 2008 Jan;19(1):56-8. doi: 10.1097/SCS.0b013e31815c8a27.
- Management of deformational plagiocephaly: repositioning versus orthotic therapy, Graham JM Jr, Gomez M, Halberg A, Earl DL, Kreutzman JT, Cui J, Guo X. J Pediatr. 2005 Feb;146(2):258-62.
- Deformational brachycephaly in supine-sleeping infants, Graham JM Jr, Kreutzman J, Earl D, Halberg A, Samayoa C, Guo X. J Pediatr. 2005 Feb;146(2):253-7.
- Real versus perceived improvements of helmet molding therapy for the treatment of plagiocephaly, Katzel EB, Koltz PF, Sbitany H, Emerson C, Girotto JA. Plast Reconstr Surg. 2010 Jul;126(1):19e-21e. doi: 10.1097/PRS.0b013e3181dab573. No abstract available.
- What is the optimal time to start helmet therapy in positional plagiocephaly? Kluba S, Kraut W, Reinert S, Krimmel M. Plast Reconstr Surg. 2011 Aug;128(2):492-8. doi: 10.1097/PRS.0b013e31821b62d6.
- Does helmet therapy influence the ear shift in positional plagiocephaly? Kluba S, Schreiber R, Kraut W, Meisner C, Reinert S, Krimmel M. J Craniofac Surg. 2012 Sep;23(5):1301-5. doi: 10.1097/SCS.0b013e31825653fa.
- Long-term treatment effectiveness of molding helmet therapy in the correction of posterior deformational plagiocephaly: a five-year follow-up, Lee RP, Teichgraeber JF, Baumgartner JE, Waller AL, English JD, Lasky RE, Miller CC, Gateno J, Xia JJ. Cleft Palate Craniofac J. 2008 May;45(3):240-5. doi: 10.1597/06-210.1. Epub 2007 Jul 17.
- A pneumatic orthotic cranial molding helmet for correcting positional plagiocephaly, Lee WT, Richards K, Redhed J, Papay FA. J Craniofac Surg. 2006 Jan;17(1):139-44.
- Helmet versus active repositioning for plagiocephaly: a three-dimensional analysis, Lipira AB, Gordon S, Darvann TA, Hermann NV, Van Pelt AE, Naidoo SD, Govier D, Kane AA. Pediatrics. 2010 Oct;126(4):e936-45. doi: 10.1542/peds.2009-1249. Epub 2010 Sep 13.
- Deformational plagiocephaly, Littlefield T. J Neurosurg Pediatr. 2010 Feb;5(2):219-21; author reply 221. doi: 10.3171/2009.7.PEDS09323. No abstract available.
- Food and Drug Administration regulation of orthotic cranioplasty, Littlefield TR. Cleft Palate Craniofac J. 2001 Jul;38(4):337-40.
- Dynamic orthotic cranioplasty: treatment of the older infant. Report of four cases, Littlefield TR, Pomatto JK, Kelly KM. Neurosurg Focus. 2000 Sep 15;9(3):e5.
- On the current incidence of deformational plagiocephaly: an estimation based on prospective registration at a single center, Littlefield TR, Saba NM, Kelly KM. Semin Pediatr Neurol. 2004 Dec;11(4):301-4.
- Evidence-based care of the child with deformational plagiocephaly, Part I: assessment and diagnosis, Looman WS, Flannery AB. J Pediatr Health Care. 2012 Jul-Aug;26(4):242-50; quiz 251-3. doi: 10.1016/j.pedhc.2011.10.003.
- Nonsynostotic occipital plagiocephaly: factors impacting onset, treatment, and outcomes, Losee JE, Mason AC, Dudas J, Hua LB, Mooney MP. Plast Reconstr Surg. 2007 May;119(6):1866-73.
- Head shape measurement standards and cranial orthoses in the treatment of infants with deformational plagiocephaly, McGarry A, Dixon MT, Greig RJ, Hamilton DR, Sexton S, Smart H. Dev Med Child Neurol. 2008 Aug;50(8):568-76. doi: 10.1111/j.1469-8749.2008.03017.x. Review. Full text
- Head orthesis therapy in infants with unilateral positional plagiocephaly: an interdisciplinary approach to broadening the range of orthodontic treatment, Meyer-Marcotty P, Böhm H, Linz C, Kunz F, Keil N, Stellzig-Eisenhauer A, Schweitzer T. J Orofac Orthop. 2012 Apr;73(2):151-65. doi: 10.1007/s00056-011-0070-z. Epub 2012 Mar 4.
- Deformational plagiocephaly and orthotic treatment: indications and limitations, Mortenson P, Steinbok P, Smith D. Childs Nerv Syst. 2012 Sep;28(9):1407-12. doi: 10.1007/s00381-012-1755-3. Epub 2012 Aug 8. Review.
- Nonsurgical, nonorthotic treatment of occipital plagiocephaly: what is the natural history of the misshapen neonatal head? Moss SD. J Neurosurg. 1997 Nov;87(5):667-70.
- Analysis of posterior plagiocephaly: deformational versus synostotic, Mulliken JB, Vander Woude DL, Hansen M, LaBrie RA, Scott RM. Plast Reconstr Surg. 1999 Feb;103(2):371-80.
- The infant with a misshapen head, Nield LS, Brunner MD, Kamat D. Clin Pediatr (Phila). 2007 May;46(4):292-8. doi: 10.1177/0009922806292027 Review. No abstract available.
- Plagiocephaly and awareness, prevention and treatment, Otway C. Community Pract. 2008 Apr;81(4):38-40. Review. No abstract available.
- Comparison of infant head shape changes in deformational plagiocephaly following treatment with a cranial remolding orthosis using a noninvasive laser shape digitizer, Plank LH, Giavedoni B, Lombardo JR, Geil MD, Reisner A. J Craniofac Surg. 2006 Nov;17(6):1084-91.
- Diagnosis and management of deformational plagiocephaly, Robinson S, Proctor M. J Neurosurg Pediatr. 2009 Apr;3(4):284-95. doi: 10.3171/2009.1.PEDS08330. Review.
- Comparison of a modifiable cranial cup versus repositioning and cervical stretching for the early correction of deformational posterior plagiocephaly, Rogers GF, Miller J, Mulliken JB. Plast Reconstr Surg. 2008 Mar;121(3):941-7. doi: 10.1097/01.prs.0000299938.00229.3e.
- Management of positional plagiocephaly, Saeed NR, Wall SA, Dhariwal DK. Arch Dis Child. 2008 Jan;93(1):82-4. Review. No abstract available. Full text
- Three-dimensional photographic analysis of outcome after helmet treatment of a nonsynostotic cranial deformity, Schaaf H, Malik CY, Streckbein P, Pons-Kuehnemann J, Howaldt HP, Wilbrand JF. J Craniofac Surg. 2010 Nov;21(6):1677-82. doi: 10.1097/SCS.0b013e3181f3c630.
- Helmet treatment of deformational plagiocephaly: the relationship between age at initiation and rate of correction, Seruya M, Oh AK, Taylor JH, Sauerhammer TM, Rogers GF. Plast Reconstr Surg. 2013 Jan;131(1):55e-61e. doi: 10.1097/PRS.0b013e3182729f11.
- Cosmetic and cognitive outcomes of positional plagiocephaly treatment, Shamji MF, Fric-Shamji EC, Merchant P, Vassilyadi M. Clin Invest Med. 2012 Oct 6;35(5):E266.
- What is the role of helmet therapy in positional plagiocephaly? Singh A, Wacogne I. Arch Dis Child. 2008 Sep;93(9):807-9. doi: 10.1136/adc.2007.121731. Review. No abstract available. Full text
- Long-term outcome of infants with positional occipital plagiocephaly, Steinbok P, Lam D, Singh S, Mortenson PA, Singhal A. Childs Nerv Syst. 2007 Nov;23(11):1275-83. Epub 2007 Jun 6. PDF
- Deformational plagiocephaly associated with ocular torticollis: a clinical study and literature review, Stevens P, Downey C, Boyd V, Cole P, Stal S, Edmond J, Hollier L. J Craniofac Surg. 2007 Mar;18(2):399-405. Review.
- Outcome analysis of helmet therapy for positional plagiocephaly using a three-dimensional surface scanning laser, Thompson JT, David LR, Wood B, Argenta A, Simpson J, Argenta LC. J Craniofac Surg. 2009 Mar;20(2):362-5. doi: 10.1097/SCS.0b013e3181992382.
- Torticollis and plagiocephaly in infancy: therapeutic strategies, van Vlimmeren LA, Helders PJ, van Adrichem LN, Engelbert RH. Pediatr Rehabil. 2006 Jan-Mar;9(1):40-6. Review.
- Helmet therapy in infants with positional skull deformation: randomised controlled trial, van Wijk RM, van Vlimmeren LA, Groothuis-Oudshoorn CG, Van der Ploeg CP, Ijzerman MJ, Boere-Boonekamp MM. BMJ. 2014 May 1;348:g2741. doi: 10.1136/bmj.g2741. Full text
| Further reading |
Deep learning-based detection of anthropometric landmarks in 3D infants head models, Helena R. Torres, Bruno Oliveira, Fernando Veloso, Mario Ruediger, Wolfram Burkhardt, António Moreira, Nuno Dias, Pedro Morais, Jaime C. Fonseca, and João L. Vilaça. Proc. SPIE 10950, Medical Imaging 2019: Computer-Aided Diagnosis, 1095034 (13 March 2019); doi: 10.1117/12.2512196
Automatic strategy for extraction of anthropometric measurements for the diagnostic and evaluation of deformational plagiocephaly from infant’s head models, Bruno Oliveira, Helena R. Torres, Fernando Veloso, Estela Vilhena, Nuno F. Rodrigues, Jaime C. Fonseca, Pedro Morais, and João L. Vilaça. Proc. SPIE 10950, Medical Imaging 2019: Computer-Aided Diagnosis, 109500A (13 March 2019); doi: 10.1117/12.2512782
Effect of head orthoses on skull deformities in positional plagiocephaly: Evaluation of a 3-dimensional approach, Dörhage KWW, Wiltfang J, von Grabe V, Sonntag A, Becker ST, Beck-Broichsitter BE. J Craniomaxillofac Surg. 2018 Jun;46(6):953-957. doi: 10.1016/j.jcms.2018.03.013. Epub 2018 Mar 29.
Preventing deformational plagiocephaly through parent guidance: a randomized, controlled trial, Aarnivala H, Vuollo V, Harila V, Heikkinen T, Pirttiniemi P, Valkama AM. Eur J Pediatr. 2015 Sep;174(9):1197-208. doi: 10.1007/s00431-015-2520-x. Epub 2015 Apr 1.
Three-dimensional analysis of cranial growth from 6 to 12 months of age, Meyer-Marcotty P, Böhm H, Linz C, Kochel J, Stellzig-Eisenhauer A, Schweitzer T. Eur J Orthod. 2014 Oct;36(5):489-96. doi: 10.1093/ejo/cjt010. Epub 2013 Mar 15. Full text
Cranial molding helmet therapy and establishment of practical criteria for management in Asian infant positional head deformity, Aihara Y, Komatsu K, Dairoku H, Kubo O, Hori T, Okada Y. Childs Nerv Syst. 2014 Sep;30(9):1499-509. doi: 10.1007/s00381-014-2471-y. Epub 2014 Jun 26. PDF
Positional plagiocephaly: an analysis of the literature on the effectiveness of current guidelines, Shweikeh F, Nuño M, Danielpour M, Krieger MD, Drazin D. Neurosurg Focus. 2013 Oct;35(4):E1. doi: 10.3171/2013.8.FOCUS13261. Review.