
The etiology of pectus carinatum involves overgrowth of costal cartilage and undergrowth of ribs

| Fig. 3. Measurement of the full length of the rib. |
| A. Three-dimensional volume rendering (VR) image is reconstructed automatically with a commercially available reconstruction program (Aquarius iNtuition Ver.4.4.6 TeraRecon, Foster City, CA). Unnecessary regions are manually deleted. |
| B. The full length of the left 4th rib is semiautomatically traced using the curved MPR technique with manual correction. |
| C. The tracing line passes through the center of rib. |
| D. The full length of the rib is measured by electronic caliper. |
| Purpose |
We compared the length of costal cartilage and rib between patients with symmetric pectus carinatum and controls without anterior chest wall protrusion, using a 3-dimensional (3D) computed tomography (CT) to evaluate whether the overgrowth of costal cartilage exists in patients with pectus carinatum.
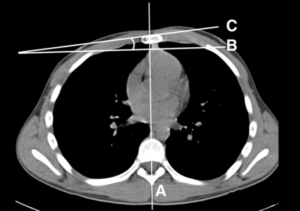
Fig. 1. Measurement of the sternal rotation angle.
| Subjects and methods |
Twenty-six patients with symmetric pectus carinatum and matched twenty-six controls without chest wall protrusion were enrolled. We measured the full lengths of the 4th–6th ribs and costal cartilages using 3-D volume rendering CT images and the curved multiplanar reformatted (MPR) techniques.
The lengths of ribs and costal cartilages, the summation of rib and costal cartilage lengths, and the costal index [length of cartilage/length of rib * 100 (%)] were compared between the patients group and the control group at 4th–6th levels.
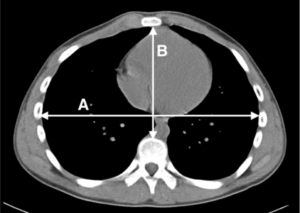
Fig. 2. Measurement of the Haller index.
| Results |
The lengths of costal cartilage in patient group were significantly longer than those of control group at 4th, 5th and 6th rib level. The lengths of ribs in patient group were significantly shorter than those of control group at 4th, 5th and 6th rib level.
The summations of rib and costal cartilage lengths were not longer in patients group than in control group. The costal indices were significantly larger in patients group than in control groups at 4th, 5th and 6th rib level.
| Conclusion |
In patients with symmetric pectus carinatum, the lengths of costal cartilage were longer but the lengths of rib were shorter than those of controls.
These findings may supports that the overgrowth of costal cartilage was not the only factor responsible for pectus carinatum.
| References |
The etiology of pectus carinatum involves overgrowth of costal cartilage and undergrowth of ribs, Chul Hwan Park, Tae Hoon Kim, Seok Jin Haam, Inhwan Jeon, Sungsoo Lee. Journal of Pediatric Surgery 49 (2014) 1252–1258. DOI: http://dx.doi.org/10.1016/j.jpedsurg.2014.02.044