
Plantar fasciitis: A new take on custom foot orthoses
The medical literature generally supports the use of foot orthoses for management of plantar fasciitis symptoms, but evidence regarding specific orthotic designs is inconclusive. Early research suggests a temporary custom foot orthosis may be an effective treatment option.
 Caryn Doggett DPT, Michelle Drak DPT, and Robert Boyles PT DSc OCS, Lower Extremity Review July 2011
Caryn Doggett DPT, Michelle Drak DPT, and Robert Boyles PT DSc OCS, Lower Extremity Review July 2011
Plantar fasciitis (PF), also referred to as heel pain syndrome, jogger’s heel, tennis heel, and calcaneodynia, is clinically defined as pain and tenderness under the heel during weightbearing leading to a limitation of activities. In some individuals it can be a source of pain for months and even years PF is the most common foot complaint in the U.S., affecting approximately 10% of people during their lifetime. It accounts for more than 1 million annual physician visits in the U.S., and is the most common foot condition seen in outpatient physical therapy clinics.
The plantar fascia is a thick fibrous connective tissue that provides dynamic shock absorption and static support of the longitudinal arch. Three primary bands make up the plantar fascia. The central band originates at the medial tubercle of the calcaneus and inserts into the proximal phalanx of toes 2 through 5. The lateral and medial bands originate from the abductor digiti minimi and abductor hallucis muscles, respectively, and are continuous with the central band and dorsal fascia.
Symptoms of PF are usually insidious and include periods of sharp pain, generally experienced with the first step in the morning or after prolonged periods of non-weightbearing activities. Symptoms may also manifest as a dull discomfort or deep ache at the origin of the plantar fascia near the inferior medial calcaneus.
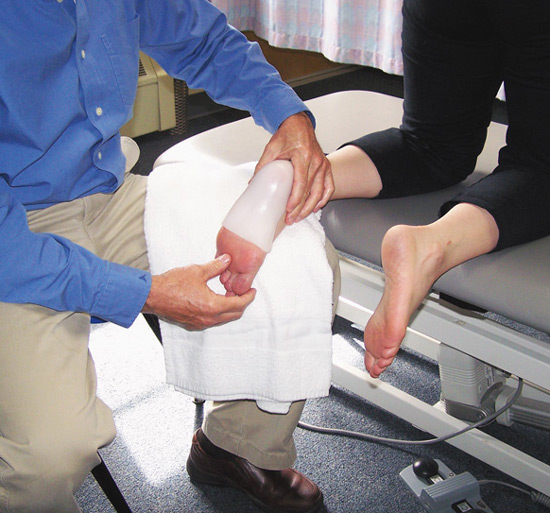
Figure 1. A temporary thermoplastic custom foot orthosis was casted in a plantar flexed and inverted position.
Evidence for PF treatment
The majority of past research has viewed PF as an inflammatory disorder thought to result from microtearing of the plantar fascia. New evidence, however, shows no inflammatory properties present in histological studies of individuals with chronic PF, but, rather, suggests PF is a degenerative condition affecting the collagen fibers. This new evidence may cause practitioners to reconsider anti-inflammatory pharmaceutical management of chronic cases, which has traditionally been the first line of treatment.
Although the exact etiology of PF is unclear, most sources agree that it results from overuse secondary to various anatomical, environmental, and biomechanical risk factors. These may include pes planus, pes cavus, limited ankle dorsiflexion, obesity, prolonged weightbearing activities, inadequate stretching, poor footwear, trauma, weak plantar flexor muscles, and excessive subtalar joint pronation. Among these factors, limited ankle dorsiflexion is associated with the highest odds ratio for developing PF (23.3, confidence interval, 4.3 to 124.4).
Due to the multifactorial nature of PF, clinicians must consider various factors when choosing a treatment approach for individual patients. The first form of treatment is general education from the primary care physician regarding pain-free activities and possible etiologies. If pain does not resolve in four to six weeks, the patient may be referred to a physical therapist, podiatrist, or foot specialist for any of a number of additional treatments. These may include electrophysical agents, shockwave therapy, non-steroidal anti-inflammatory drugs, manual therapy, stretching, taping, night splints, corticosteroid injections, foot orthoses, or combined treatments. Surgery is an option for those with recalcitrant PF.
Evidence regarding foot orthoses
Foot orthoses are often used for the treatment of PF. This line of treatment is supported by both patient reports and biomechanical theory. Studies have demonstrated that excessive pronation and lower arch shape, in addition to repetitive trauma and overuse, can increase tension on the plantar fascia, leading to pain. Orthoses are believed to reduce the strain on the plantar fascia and provide foot support. This should lead to an overall decrease in medial heel and arch pain.
Continue reading in Lower Extremity Review
Also see
A Prospective Randomized Trial Using Four Treatment Modalities for the Treatment of Plantar Fasciitis, Gerald T. Kuwada DPM NMD. The Foot and Ankle Online Journal 4 (8): 1. August 11, 2011. doi: 10.3827/faoj.2011.0408.0001
Effects of a Custom-Fit Orthosis for Plantar Fasciitis at Multidisciplinary Rehabilitation Research Centre, Regina SK