
Nonsynostotic deformational plagiocephaly: Understand, screen, and intervene
DP has a short window of opportunity for intervention while the skull bones are malleable; after age 24 months, the cranial sutures are generally fused.

0rthomerica
Laura C. Steinmann RN, Samantha Elaine Struthers PhD OTR/L, Medscape June 17, 2014
| Introduction to deformational plagiocephaly |
Deformational plagiocephaly (DP) refers to asymmetry of the infant skull characterized by flattening or deformation. DP can include facial and neck asymmetry. Congenital muscular torticollis (CMT) is often involved and should be ruled out as a causative factor for DP. In contrast to craniosynostosis, which occurs when 1 or more cranial sutures are prematurely fused (stenosed), nonsynostotic DP is not related to bone/skull fusion. Craniosynostosis warrants surgical correction and therefore must also be ruled out as a causative factor for DP.
Craniosynostosis may occur in conjunction with accompanying syndromes (eg, genetic or chromosomal disorders, spinal disease, etc.), and these conditions should be recognized early and monitored closely by a multidisciplinary healthcare team. This report will refer to nonsynostotic DP as DP and will review it. Craniosynostosis is not discussed in this report.
DP has a short window of opportunity for intervention while the skull bones are malleable; after age 24 months, the cranial sutures are generally fused. Parents of newborns should receive preventive counseling (anticipatory guidance) and information on positioning the infant as recommended by the American Academy of Pediatrics (AAP).
Ideally, information on a positioning program is provided at hospital discharge and no later than at the 1-month well-child visit. Infants should be screened for skull deformity at each well-child visit to detect deformities that occur after birth, as delineated in Bright Futures: Recommendations for Preventive Pediatric Health Care. These guidelines recommend a skull deformity health risk assessment in babies up to 1 year of age; however, we have documented head shape changes in children up to age 24 months.
For infants with DP, parents should be instructed to follow a 2- to 3-month course of repositioning; if no improvement is seen, AAP recommends referral to a craniofacial specialist by age 4-6 months to diagnose and direct subsequent management, which may include molding helmets or surgery.
Craniofacial asymmetry may be obvious or subtle. Knowing when to monitor and when to refer for management requires an ability to recognize early DP, distinguish DP from craniosynostosis, and recognize improvement or worsening of head asymmetry in an infant.
The term “plagiocephaly” is commonly used to describe any head shape dysmorphology. An Internet search for the term finds many different names including facial scoliosis, flat head syndrome, parallelogram head, and others. European studies refer to frontal and occipital plagiocephalies. Parents and caregivers may refer to DP as a “flat spot.” Researchers and health insurance policies commonly use the terms “positional” or “acquired” plagiocephaly. These terms imply that DP can be avoided and may lack veracity given research suggesting multiple extrinsic and intrinsic contributing factors.
Head shape deformities, particularly DP, are not well understood by healthcare providers and payers, who classify this as low-priority, a minor cosmetic issue, or simply the result of positioning practices, and who do not recognize the need for intervention. Parents may assume guilt and feel blamed because their positioning practices allowed their child to acquire the condition, and may shun treatment because they are embarrassed. The terms “positional” or “acquired” plagiocephaly do not serve the best interests of families, and the term “deformational plagiocephaly” is preferred.
| What factors put a child at risk? |
Why are some children vulnerable to head shape asymmetry? Factors involved may be extrinsic (modifiable, environmental) or intrinsic (not modifiable, genetic). DP occurs in susceptible infants who are placed, for prolonged periods, in a position that puts pressure on their moldable skulls, causing deformation. Spontaneous movement may be inhibited prenatally in a restricted uterine environment and/or postnatally in a carrier, car seat, swing, stroller, or tight clothing; in neonatal intensive care units; or from cultural practices such as cradle boards or swaddling.
AAP provides guidelines for a safe infant sleeping environment and recommends that infants sleep in the supine position (as detailed in the National Institutes of Health’s Safe To Sleep® campaign). This has been cited as a cause of increased specialist referrals related to DP, although it is not clear whether the incidence of DP is rising or just being recognized and reported more often.
Environmental factors do not explain all possible contributing causes of nonsynostotic DP. Intrinsic factors include skeletal and neurocranial growth, the sutures and fontanels (size, location, patency, and ability to accommodate bone movement), and the health and integrity of the associated cranial and neck musculature, ligaments, synovial joints, tendons, and fascia (connective tissue). Lin and colleagues demonstrated that genetic growth factors within cranial sutures may have varying rates of osteoblast (bone) development causing sutures to ossify unevenly. Insufficient levels of vitamin D may reduce bone mineralization and strength in susceptible children. Oh and colleagues found a major role of CMT in the development of DP and showed a positive correlation between the degree of cervical imbalance and the severity of cranial asymmetry. CMT is a common pediatric musculoskeletal condition in which damage to a neck muscle causes it to shorten; this, in turn, causes the head to tilt toward the side of the affected muscle, with neck rotation to the opposite side.
An infant’s first gross motor milestone is the development of head and neck control in the supine and prone positions and in supported sitting. DP and CMT can interfere with head rotation because the child cannot easily roll off the flattened occipitoparietal area; this, in turn, may delay a milestone in the developmental sequence of rolling over and fixing the gaze at midline. CMT is associated with cranial asymmetry as are 2 other musculoskeletal disorders, scoliosis and developmental dysplasia of the hip.
| DP and related conditions |
Clinicians regularly screen for growth and development, vision, hearing, and oral health; a growing body of research provides evidence that these outcomes can be affected by craniofacial misalignment. Craniofacial asymmetry may be a factor in functional deficits involving visual fields, auditory processing, temporomandibular asymmetry, and dentoskeletal dysmorphology. Oral health risk assessment is recommended at 6- and 9-month well-child visits. Occlusal development starts with the eruption of the first primary tooth at around age 6 months; maxillary or mandibular asymmetries can affect proper dental occlusion and, thus, oral health.
Research supports a correlation between DP and developmental delays in cognition, language, and motor skills. Children with pre-existing neurodevelopmental vulnerability are at higher risk of developing DP. In addition to being a diagnosis, DP may be a symptom or physical marker of neurodevelopmental risk in children younger than age 6 months and often is evident before the child is easily evaluated by other markers, providing precious time for earlier intervention.
Collett and colleagues found that children with a history of DP plus developmental delay at initial diagnosis still have a measurable delay at age 36 months; they suggested that infants meeting diagnostic criteria for DP should be routinely screened and monitored for neurodevelopmental problems. US federal law mandates early identification of children with developmental disabilities. Although discussing potential neurodevelopmental problems with parents is a challenge, most children do not outgrow developmental problems; when a delay is detected, the most cautious and careful approach is not to defer but rather to refer the child promptly for evaluation and treatment.
Correlation does not imply causation. AAP does not acknowledge a causal link between DP and developmental delay, temporomandibular asymmetry, Otitis media, visual development, scoliosis, or hip dislocation. Insurance policies acknowledge that “limited clinical evidence suggests plagiocephaly may be associated with future ocular and/or oral abnormalities” but also question whether treatment provides a future health benefit or merely a cosmetic effect.
Hutchinson and colleagues found that the point prevalence of plagiocephaly halved between 1 and 2 years of age, suggesting that without treatment, 50% of diagnosed head shape dysmorphology may normalize during early childhood; however, Yoo and colleagues found that nonsynostotic DP and resulting craniofacial deformities do not spontaneously improve. The data vary, and providers may infer that in many cases children will outgrow DP without intervention; nevertheless, in all cases one cannot predict which child with DP may have long-term health sequelae. From an epidemiologic perspective, it is important to identify and address modifiable factors that place an infant at risk for DP and potentially reduce its prevalence and the long-term cost of management.
| Anatomy of the head and neck |
To understand DP, it is helpful to quickly review cranial bones, sutures, fontanels, and neck muscles and consider how they relate to and articulate with each other. Figure 1 provides an overview of the infant cranial bones, sutures, and fontanels primarily discussed in this report. The infant skull is made up of bone plates; the larger of these are the frontal, temporal, parietal, and occipital bones of the skull, and the sphenoid, zygomatic, maxilla, and mandible bones of the face.
Between the bone plates are fibrous sutures (metopic, coronal, sagittal, lambdoid, squamosal) and fontanels (anterior, posterior, sphenoid, mastoid). During birth, the open sutures and fontanels allow the bone plates to slide over each other to ease passage of the head through the birth canal. Growth of the neurocranium is largely determined by growth of the brain, which develops rapidly and reaches 90% of adult head size by age 1 year; after 24 months, the bones have interlocked at the sutures. Premature ossification of the sutures, or craniosynostosis, will inhibit proper cranial bone movement and skull growth.
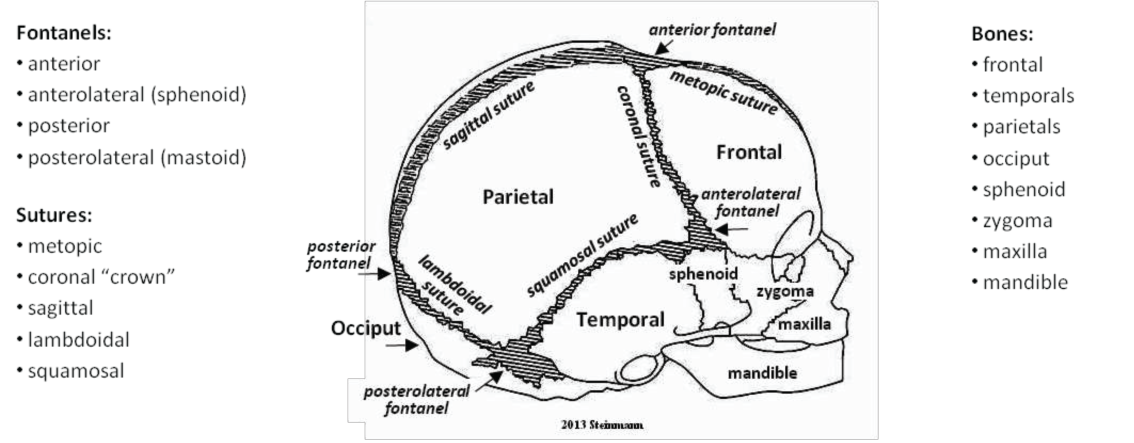
| Figure 1. The bones, sutures, and fontanels of the face and skull. Steinmann, et al. 2014 |
CMT is typically characterized by a head tilt to one side or lateral neck flexion, with the neck rotated to the opposite side because of unilateral shortening or fibrosis of the sternocleidomastoid muscle (Figure 2). A shoulder hike may occur on the affected side depending on the degree of neck rotation.
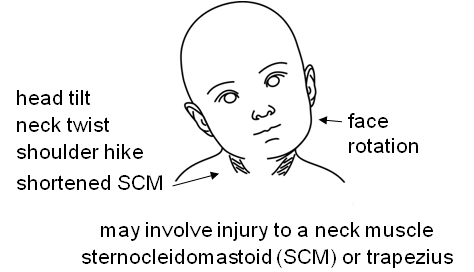
| Figure 2. Torticollis neck symmetry. American Nurse today |
In our clinical experience, each child’s head asymmetry is individual, and the movement of skull and facial bones can be unpredictable, uneven, and often based on unknown contributing factors. In some children, lying supine may cause the occiput to flatten and widen; the widened occiput may affect adjacent bones (parietals, temporals) on one or both sides of the skull. In others, side lying may affect the parietals as well as the occiput.
Cranial bones may move forward (anterior), upward, or a combination of both. An upward push may increase the posterior skull height, called vaulting, and may also affect the frontal bones (forehead). An anterior push from the occiput or parietals may affect the temporal bones on one or both sides, which may in turn cause an ear to shift forward or lead to facial bone involvement (ie, forehead, orbit, sphenoid, zygoma, maxilla, mandible). Facial bone involvement may be irregular and seemingly random; for example, there may be apparent forehead bossing (protrusion) and cheek bossing but no apparent involvement of the orbit. There may be misalignment of the eyes, nose, and chin but no apparent cheek (zygoma) bossing, or vice versa. It is especially important to intervene when a child presents with facial bone involvement.
| Screening: An important early step |
Developing a clinical pathway to treat head shape deformity is complicated by the seemingly subjective nature of diagnosis. Nonetheless, clinicians can develop skills to visualize and assess head shape and integrate a skull deformity health risk assessment into pediatric practice. AAP guidelines for well-child visits outlined in Bright Futures include both screening and surveillance in order to detect potential sensory integration problems. Using only clinical impressions (surveillance) rather than formal screenings leads to underdetection and reduces the possibility of early intervention, and waiting until a child misses a developmental milestone may result in delayed recognition of a child’s needs. The goals are to recognize DP and CMT, optimize interventions, and improve children’s health outcomes.
The main steps involved in head shape screening are to: visualize alignment, level, and proportion of head, face, and neck; measure head circumference, width, length, cranial index, and cranial vault asymmetry; diagnose by determining shape (based on 3 head shapes commonly related to DP); and classify, document, and refer as needed.

| Figure 3. Cranial views of a typically developing child. Steinmann, et al. 2014 |
Imagine horizontal and vertical lines to check the head for alignment, level, and proportion.
- Alignment: imagine a vertical line in the sagittal plane, anterior from the anterior fontanel down to the nose, subnasion, chin, and neck;and posterior from the vertex down to the fontanel, occiput, and neck. Imagine a line in the coronal plane connecting the ears.
- Level: imagine horizontal lines across the vertex and forehead and connecting facial features (eyebrows, eyes, ears, cheeks, chin) and neck; note if level, even.
- Proportion: imagine lines dividing the skull into quadrants; note if quadrants are relatively equal in volume.

| Figure 4. Parameters for assessing alignment, level, and proportion of the head and face. Steinmann, et al. 2014 |
Craniofacial anomalies may be subtle and not readily apparent to the untrained eye. Palpate the skull and identify bones, suture lines, fontanels, prominent points, and flat areas; one can practice by palpating and identifying their own skull bones and suture lines.
Clinicians may not have the equipment to measure or the time to take measurements; however, based on clinical presentation, one can visually screen, document, and refer.
| Measure |
Head symmetry is measured using cranial anthropometric landmark guidelines, calipers (slide or spreading), and a head circumference tape. Head circumference is an important parameter; however, it is not an indicator of plagiocephaly, either synostotic or nonsynostotic, because in both types the absolute head circumference may be normal despite the skull being misshapen. Clinicians should consider screening for head shape at the same time head circumference is measured at every well-child visit.
Five primary measurement parameters are included in this report for head shape determination:
- Head circumference: measure from glabella (prominent point between eyebrows where supraorbital ridges join) around the opisthocranion (most prominent posterior point on the occiput).
- Head width: side-to-side measurement; use sliding caliper across top of skull from eurion (most lateral point on parietal region) to opposite eurion.
- Head length: anterior-posterior measurement; use sliding caliper across top of skull from glabella to opisthocranion.
- Cranial Index (CI): also referred to as cephalic index, cranial ratio, cephalic ratio; a measurement to categorize head shapes in populations. CI = width ÷ length x 100. We use the following ranges:
- Cranial vault asymmetry (CVA): also referred to as diagonal difference, oblique diagonal difference, or transcranial difference. CVA is the difference between 2 diagonal measurements (frontozygomaticus to opposite eurion). Note that CVA will be symmetric in symmetric brachy-, and dolichocephaly.

| Figure 5. Cranial vault symmetry and asymmetry. Steinmann, et al. 2014 |
- Hutchinson (mild, 3-10 mm; moderate, 10-12 mm; severe, >12 mm);
- Yoo (mild, 6-10 mm; moderate, 11-15 mm, severe, >16 mm);
- Mulliken (severe, 10-12 mm); and
- Loveday and Graham (severe, >10 mm).
- Insurance policies differ slightly but generally require a severity of 10-12 mm, as a minimum to approve treatment of DP.
Few skulls are perfectly symmetric, and even symmetric skulls may have minor variations of alignment of the facial features (eyes, eyebrows, nose, ears, or chin) but not usually more than a 3- to 6-mm difference, depending on clinical presentation. In our clinic, facial feature differences greater than 6 mm or CVA greater than 12 mm are generally of concern and require follow-up.
| Diagnose |
Normocephaly is an overall relatively symmetric head shape with measurement parameters that are within normal limits (WNL). The 3 main head shapes commonly related to nonsynostotic DP are:
- Plagiocephaly
- Brachycephaly, both symmetric and asymmetric, and
- Dolichocephaly, both symmetric and asymmetric. Dolichocephaly (commonly called scaphocephaly) is the term that correlates with ICD-10 codes.
| 1. Plagiocephaly |
- CI >76% to <90%, asymmetric head shape, occipitoparietal flattening, ear misalignment
- May affect temporal, parietal, and/or frontal bones and facial symmetry
- May occur alone or in combination with brachycephaly or dolichocephaly
- May result from premature fusion of one or both coronal sutures or rarely the lambdoid sutures

| Figure 6. Plagiocephaly. Steinmann, et al. 2014 |
| 2. Brachycephaly |
- CI >90%, short skull, occiput flattened, widened
- May affect parietal, temporal, and/or frontal bones and facial symmetry
- May occur alone or in combination with plagiocephaly
- May result from the premature fusion of the coronal or lambdoid sutures
Symmetric brachycephaly: CVA WNL; CI not WNL; central symmetrical occipital flattening, widening; may cause steep symmetrical cranial vault; little/no ear shift
Asymmetric brachycephaly: CVA not WNL; combination plagiocephaly with widened occiput; flattening crosses occipital midline; possible anterior ear shift, frontal involvement
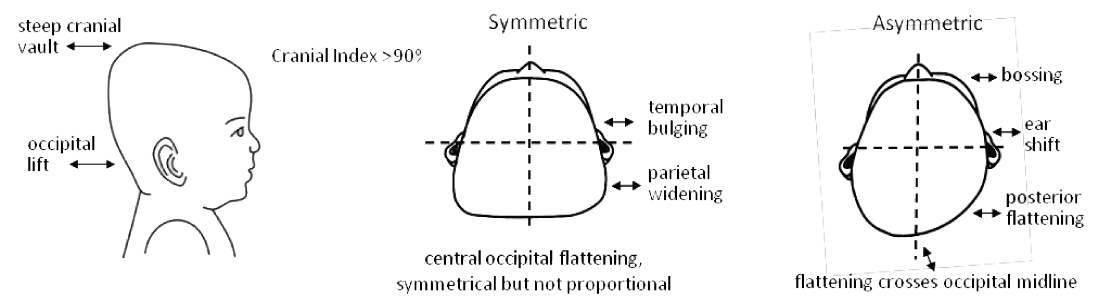
| Figure 7. Brachycephaly. Steinmann, et al. 2014 |
| 3. Dolichocephaly |
- CI <76%, long, narrow skull, affects occiput, temporal, parietal and frontal bones, may affect facial bones
- May be familial, often noted in premature babies, uterine breech position
- May result from premature fusion of the sagittal suture
Symmetric dolichocephaly: CI not WNL; CVA may be WNL; elongated skull, narrow parietals; little/no ear shift
Asymmetric dolichocephaly: CVA and CI not WNL; combination plagiocephaly with narrow skull; occipitoparietal flattening, possible anterior ear shift, frontal involvement
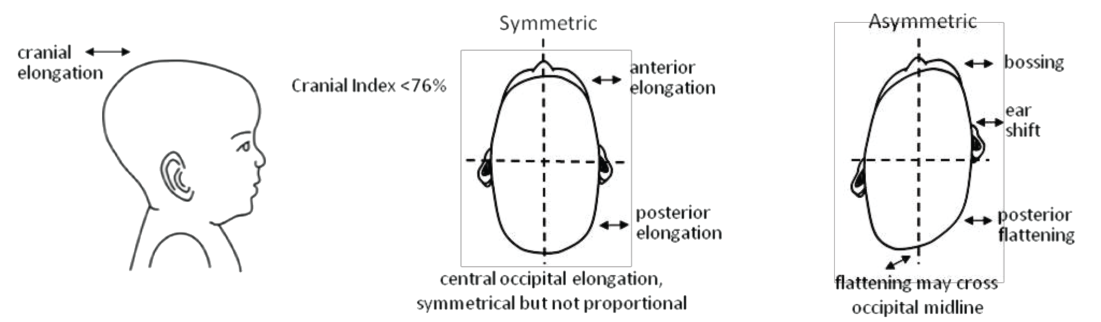
| Figure 8. Dolichocephaly. Steinmann, et al. 2014 |
| Classify and document |
A standard classification system to quantify DP has not been adopted. A differential diagnosis for skull deformities includes craniosynostosis vs a positional (deformational), nonsynostotic plagiocephaly, with or without torticollis.
Scales using mild, moderate, or severe classifications are often subjective and vary among researchers and practitioners. Several scales are worth mentioning, however. The Argenta scale is a validated tool that provides a qualitative assessment progressing from Type 1 (minimal) to Type 5 (severe). Children’s Healthcare of Atlanta (CHOA) has developed a useful classification tool called the Plagiocephaly Severity Scale that includes a scale of Levels 1-5, similar to Argenta, plus the Cranial Vault Asymmetry Index that measures CVA percentage differences to compare the child’s head shape as the child grows, independent of age-related changes in head size. Our clinic uses the CHOA scale to classify the level of asymmetry of plagiocephaly, asymmetric brachycephaly, and asymmetric dolichocephaly. The scale is less useful for symmetric brachycephaly and symmetric dolichocephaly because the dysmorphology is not symmetric but proportional.
Argenta describes 3 stages of brachycephaly demonstrating progressive deformity from Type 1 to Type 3. Measures of head shape developed by researchers over the years are slowly being incorporated into regulatory and private payer policies; with repetition and validation, these measurements become our standards.
For documentation purposes, insurance policy criteria to approve treatment of nonsynostotic DP are useful because they have fairly standard requirements and outline acceptable criteria based on accepted peer-reviewed research. One should document clinical presentation, indicate whether positioning programs were used, include anthropometric measurements, and provide a diagnosis and treatment plan. Finally, intervene as appropriate, provide education and resources, and refer to a specialist as needed.
| A Guideline for examining the head, face, and neck |
The Table details a guideline for examining the head, face, and neck, with landmark prompts for clinicians to assess cranial alignment, level, and proportion and visualize facial symmetry. Interview the parents/caregivers and ask them to describe their child’s head shape in their own words to help understand their perceptions. Document important clinical information, including current health, well-child visits, early intervention programs, and whether the child is meeting age-related milestones.
Other factors to consider include sex and birth order, pregnancy history (first child, multiple birth, gestational age), type of birth (vaginal, Caesarean section, breech, use of forceps), family history, and positioning practices. If necessary, dampen the child’s hair so it lies flat against the skull because hair often hides shape problems. Children generally do not mind when their skull is palpated, but be prepared to distract them with a toy, pacifier, bottle, or cell phone application.
| Appropriate interventions for plagiocephaly |
An appropriate intervention is based on the child’s age, clinical presentation, and diagnosis; an effective intervention will involve support and collaboration between the child’s parents or caregiver and the primary healthcare provider. Below is an overview of intervention strategies.
| Positioning program |
All newborns should begin a positioning program starting at birth. Anticipatory guidance for parents should include education on positioning programs that includes prone positioning and play, such as CHOA’s Tummy Time Tools. Some ideas to encourage turning and reaching movement in newborns include: dress in clothing that protects but allows freedom to move head, shoulders, and arms (no blanket, do not swaddle); when awake, place on a hard surface (firm mattress, play mat, rug, etc.) in a clean, safe, confined space (cot, play-pen) and alternate supine and prone positions; place toys at the baby’s side (not hanging above head) to attract attention and encourage movement; use baby seats sparingly, only when traveling or at mealtimes; alternate right/left sides for feeding and holding.
Repositioning techniques are not effective after the child is self-rolling; occipitoparietal flattening may actually interfere with this milestone because the child cannot easily roll off the flat area. Because nonsynostotic DP may be related to factors that cannot be modified, providers should not be surprised if the parents use a positioning program but do not achieve beneficial results. If no improvement is seen after a 2- to 3-month course of repositioning, AAP recommends referral to a craniofacial specialist by age 4-6 months to rule out craniosynostosis.
| Therapy for plagiocephaly |
CMT is often more obvious than DP, and clinicians may quickly refer for physical or occupational therapy. This report does not include widely available information on the types of exercises therapists use to treat DP. Physicians, physician assistants, nurse practitioners, nurse midwives, obstetric nurses, lactation specialists, or any clinician or family member should refer infants identified as having positional preference, reduced cervical range of motion, sternocleidomastoid masses, facial asymmetry, and/or plagiocephaly to the primary pediatrician and a physical therapist as soon as the asymmetry is noted.
Generally, parents can self-refer to an early intervention program or an orthotist; however, the primary healthcare provider must approve any medical intervention. The Centers for Medicare & Medicaid Services (CMS) provides a comprehensive benefit package to children, including Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) services, which under US federal law covers any service deemed medically necessary to promote a child’s healthy physical, behavioral, and emotional development.
| Cranial remolding orthoses (CROs) |
CROs are referred to by different names, such as helmets or bands, and are an orthotic brace to help align cranial bones, analogous to dental braces that help align teeth. CROs channel head growth by applying passive pressure on the prominent areas of the infant skull while leaving room for growth in the flattened areas. CROs are custom fabricated, made of rigid plastic with a soft interface material. A physician’s order is required for a CRO; an orthotist provides head shape data for parents and providers to make intervention decisions, fits the CRO, and makes adjustments as the child grows. A CRO may be used when repositioning has not helped and craniosynostosis has been ruled out. These devices are not the same as protective helmets commonly used to prevent injury for children with special needs.
The window of opportunity for CRO intervention is brief, occurring only while cranial sutures are still open. AAP recommends CROs for ages 4-12 months because of the greater malleability of the young infant skull bone and the normalizing effect of the rapid growth of the brain. The US Food and Drug Administration (FDA) regulates helmets (Class 2 medical device) and recommends CROs for infants ages 3-18 months for moderate to severe nonsynostotic positional plagiocephaly, including infants with plagiocephalic-, brachycephalic-, and scaphocephalic-shaped heads.
After age 18 months, CRO intervention requires a Letter of Medical Necessity according to FDA guidelines because correction is less likely to be effective. After the FDA provides clearance of a device, CMS sets standards; currently CMS does not have a National Coverage Determination for CROs to treat plagiocephaly or surgically corrected craniosynostosis. CROs are not indicated for children under age 3 months or for craniosynostosis or hydrocephalus; however, a CRO may be used following surgical correction of craniosynostosis. Many insurance companies approve CROs for nonsynostotic DP within criteria; they may request documentation of a positioning program trial.
Parents and caregivers should be counseled regarding their expectations of cranial remolding, the rigorous treatment regimen (helmet wear 23 hours/day, 1 hour off for bathing and for cleaning the helmet, for up to 6 months), and requirements for follow-up adjustments to assure optimal CRO fit throughout the treatment period. No data suggest that successful intervention of head shape dysmorphology using CRO will change the outcome of developmental delay, if present.
| Conclusion |
DP and craniofacial misalignment can affect health outcomes related to growth and development, vision, hearing, and oral health. As pediatric healthcare providers, we can improve health outcomes for children with DP by integrating craniofacial and neck screening into current clinical practice at well-child visits from birth to age 24 months. Head shape screening can be performed at the same time head circumference is measured. We can and should provide anticipatory guidance and education for parents and caregivers regarding infant head shape and positioning programs, be alert to identify DP and CMT at an early age, and intervene and/or refer to a specialist as needed.
Head shape assessment takes practice but can easily be learned. Collecting and reporting head shape data will enhance the evidence-based data and outcome measures so that better, more informed recommendations can be made in the future. The goals are to recognize DP and CMT, optimize interventions, and improve children’s health outcomes. Families, communities, and healthcare systems will benefit by adding head shape screening to well-child visits. We can intervene to improve their futures and ours.
Source Medscape
| References |
- Predictors of severity in deformational plagiocephaly, Oh AK, Hoy EA, Rogers GF. J Craniofac Surg. 2009 Mar;20 Suppl 1:685-9. doi: 10.1097/SCS.0b013e318193d6e5. Erratum in: J Craniofac Surg. 2009 Sep;20(5):1629-30.
- The differential diagnosis of abnormal head shapes: separating craniosynostosis from positional deformities and normal variants, Huang MH, Mouradian WE, Cohen SR, Gruss JS. Cleft Palate Craniofac J. 1998 May;35(3):204-11.
- Growth of the normal skull vault and its alteration in craniosynostosis: insights from human genetics and experimental studies, Morriss-Kay GM, Wilkie AO. J Anat. 2005 Nov;207(5):637-53. Review. Full text
- Skull deformities, Ridgway EB, Weiner HL. Pediatr Clin North Am. 2004 Apr;51(2):359-87. Review. PDF
- Prevention and management of positional skull deformities in infants, Laughlin J, Luerssen TG, Dias MS; Committee on Practice and Ambulatory Medicine, Section on Neurological Surgery. Pediatrics. 2011 Dec;128(6):1236-41. doi: 10.1542/peds.2011-2220. Epub 2011 Nov 28. Erratum in: Pediatrics. 2012 Mar;129(3):595.
- Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents, Hagan JF, Shaw JS, Duncan PM, eds. 3rd Edition. Elk Grove Village, IL: American Academy of Pediatrics; 2008. PDF
- Evidence-based care of the child with deformational plagiocephaly, Part I: assessment and diagnosis, Looman WS, Flannery AB. J Pediatr Health Care. 2012 Jul-Aug;26(4):242-50; quiz 251-3. doi: 10.1016/j.pedhc.2011.10.003.
- Cranial orthotic devices for positional or deformational plagiocephaly. Cigna Medical Coverage Policy 0056 (CareAllies). Effective date March 15, 2013. Accessed May 10, 2014.
- Deformational Plagiocephaly: Recommendations for Future Research, Littlefield, Timothy R. MS; Kelly, Kevin M. PhD. JPO Journal of Prosthetics and Orthotics: October 2004-Volume 16-Issue 4-p S59-S62. Full text
- Torticollis, facial asymmetry and plagiocephaly in normal newborns, Stellwagen L, Hubbard E, Chambers C, Jones KL. Arch Dis Child. 2008 Oct;93(10):827-31. doi: 10.1136/adc.2007.124123. Epub 2008 Apr 1.
- Impacting infant head shapes, Hummel P, Fortado D. Adv Neonatal Care. 2005;5:329-340. Abstract
- Swaddling: a systematic review, van Sleuwen BE, Engelberts AC, Boere-Boonekamp MM, Kuis W, Schulpen TW, L’Hoir MP. Pediatrics. 2007 Oct;120(4):e1097-106. Review.
- SIDS and other sleep-related infant deaths: expansion of recommendations for a safe infant sleeping environment, Task Force on Sudden Infant Death Syndrome, Moon RY. Pediatrics. 2011 Nov;128(5):e1341-67. doi: 10.1542/peds.2011-2285. Epub 2011 Oct 17. Review.
- Safe to Sleep®. National Institute of Child Health and Human Development (NICHD). Accessed June 5, 2014.
- Active counterpositioning or orthotic device to treat positional plagiocephaly? Loveday BP, de Chalain TB. J Craniofac Surg. 2001 Jul;12(4):308-13.
- Investigation into an increase in plagiocephaly in Texas from 1999 to 2007, Sheu SU, Ethen MK, Scheuerle AE, Langlois PH. Arch Pediatr Adolesc Med. 2011 Aug;165(8):708-13. doi: 10.1001/archpediatrics.2011.42. Epub 2011 Apr 4.
- Elevated levels of transforming growth factors beta 2 and beta 3 in lambdoid sutures from children with persistent plagiocephaly, Lin KY, Nolen AA, Gampper TJ, Jane JA, Opperman LA, Ogle RC. Cleft Palate Craniofac J. 1997 Jul;34(4):331-7.
- Vitamin D deficiency in children and its management: review of current knowledge and recommendations, Misra M, Pacaud D, Petryk A, Collett-Solberg PF, Kappy M; Drug and Therapeutics Committee of the Lawson Wilkins Pediatric Endocrine Society. Pediatrics. 2008 Aug;122(2):398-417. doi: 10.1542/peds.2007-1894. Review.
- Physical therapy management of congenital muscular torticollis: an evidence-based clinical practice guideline: from the Section on Pediatrics of the American Physical Therapy Association, Kaplan SL, Coulter C, Fetters L. Pediatr Phys Ther. 2013 Winter;25(4):348-94. doi: 10.1097/PEP.0b013e3182a778d2. Review.
- Motor Assessment of the Developing Infant, Piper MC, Darrah J. Philadelphia, PA: Saunders; 1994:96-97. Hardcover ISBN: 9780721643076
- 3-D analysis of facial asymmetry in children with hip dysplasia, Tolleson SR, Kau CH, Lee RP, English JD, Harila V, Pirttiniemi P, Valkama M. Angle Orthod. 2010 Jul;80(4):519-24. doi: 10.2319/082009-472.1.
- Ultrasonographic study of the coexistence of muscular torticollis and dysplasia of the hip, Tien YC, Su JY, Lin GT, Lin SY. J Pediatr Orthop. 2001 May-Jun;21(3):343-7.
- Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening, Council on Children With Disabilities; Section on Developmental Behavioral Pediatrics; Bright Futures Steering Committee; Medical Home Initiatives for Children With Special Needs Project Advisory Committee. Pediatrics. 2006 Jul;118(1):405-20. Erratum in: Pediatrics. 2006 Oct;118(4):1808-9.
- Eye examination in infants, children, and young adults by pediatricians. Committee on Practice and Ambulatory Medicine, Section on Ophthalmology; American Association of Certified Orthoptists; American Association for Pediatric Ophthalmology and Strabismus; American Academy of Ophthalmology. Pediatrics. 2003;111:902-907. Accessed May 30, 2014.
- Clinical Report—Hearing Assessment in Infants and Children: Recommendations Beyond Neonatal Screening, Harlor AD Jr, Bower C; Committee on Practice and Ambulatory Medicine; Section on Otolaryngology-Head and Neck Surgery. Pediatrics. 2009;124:1252-1263. PDF
- Visual field defects in deformational posterior plagiocephaly, Siatkowski RM, Fortney AC, Nazir SA, Cannon SL, Panchal J, Francel P, Feuer W, Ahmad W. J AAPOS. 2005 Jun;9(3):274-8.
- Auditory ERPs reveal brain dysfunction in infants with plagiocephaly, Balan P, Kushnerenko E, Sahlin P, Huotilainen M, Näätänen R, Hukki J. J Craniofac Surg. 2002 Jul;13(4):520-5; discussion 526.
- Atypical auditory event-related potentials in preterm infants during the first year of life: a possible sign of cognitive dysfunction? Fellman V, Kushnerenko E, Mikkola K, Ceponiene R, Leipala J, Naatanen R. Pediatr Res. 2004 Aug;56(2):291-7. Epub 2004 Jun 4.
- Anthropometric analysis of mandibular asymmetry in infants with deformational posterior plagiocephaly, St John D, Mulliken JB, Kaban LB, Padwa BL. J Oral Maxillofac Surg. 2002 Aug;60(8):873-7. Erratum in: J Oral Maxillofac Surg. 2005 Mar;63(3):419.
- Three-dimensional computed tomography cephalometry of plagiocephaly: asymmetry and shape analysis, Netherway DJ, Abbott AH, Gulamhuseinwala N, McGlaughlin KL, Anderson PJ, Townsend GC, David DJ. Cleft Palate Craniofac J. 2006 Mar;43(2):201-10.
- Mandibular dysmorphology in unicoronal synostosis and plagiocephaly without synostosis, Kane AA, Lo LJ, Vannier MW, Marsh JL. Cleft Palate Craniofac J. 1996 Sep;33(5):418-23.
- Guideline on management of the developing dentition and occlusion in pediatric dentistry. American Academy of Pediatric Dentistry (AAPD). Adopted 1990. Revised 2009. Accessed June 5, 2014.
- Long-term developmental outcomes in patients with deformational plagiocephaly, Miller RI, Clarren SK. Pediatrics. 2000 Feb;105(2):E26.
- Motor development of infants with positional plagiocephaly, Kennedy E, Majnemer A, Farmer JP, Barr RG, Platt RW. Phys Occup Ther Pediatr. 2009;29(3):222-35.
- Case-control study of neurodevelopment in deformational plagiocephaly, Speltz ML, Collett BR, Stott-Miller M, Starr JR, Heike C, Wolfram-Aduan AM, King D, Cunningham ML. Pediatrics. 2010 Mar;125(3):e537-42. doi: 10.1542/peds.2009-0052. Epub 2010 Feb 15. Full text
- Neurodevelopmental delays in children with deformational plagiocephaly, Kordestani RK, Patel S, Bard DE, Gurwitch R, Panchal J. Plast Reconstr Surg. 2006 Jan;117(1):207-18; discussion 219-20.
- Development at age 36 months in children with deformational plagiocephaly, Collett BR, Gray KE, Starr JR, Heike CL, Cunningham ML, Speltz ML. Pediatrics. 2013 Jan;131(1):e109-15. doi: 10.1542/peds.2012-1779. Epub 2012 Dec 24. Full text
- Neurodevelopmental implications of “deformational” plagiocephaly, Collett B, Breiger D, King D, Cunningham M, Speltz M. J Dev Behav Pediatr. 2005 Oct;26(5):379-89. Review. Full text
- Individuals with Disabilities Education Act (IDEA). Public Law 101-476,104 Statute 1142. Amended 2004, Public Law 108-446. CFR Title 34 Parts 300, 301. US Department of Education. PDF
- Accurate developmental screening saves, Glascoe FP. Pediatric News Digital Network. International Medical News Group, LLC. August 1, 2007. Accessed March 1, 2014.
- Plagiocephaly & craniosynostosis treatment. Protocol ORT010: UnitedHealthCare Clinical Policy. December 10, 2012. Accessed May 10, 2014.
- Plagiocephaly and craniosynostosis treatment. UnitedHealthCare Oxford. Clinical Policy Number Surgery 067.5 T2: January 1, 2013. Accessed May 10, 2014.
- Plagiocephaly treatments, dynamic orthotic cranioplasty and soft helmets. HealthNet National Medical Policy. Policy Number NMP311: Updated March 2012. Accessed May 10, 2014.
- Adjustable cranial orthoses for positional plagiocephaly and cranial synostoses. Blue Cross Blue Shield of Vermont. April 16, 2012. Accessed May 10, 2014.
- Cranial orthotic devices for positional plagiocephaly. AmeriHealth Caritas. Clinical Policy Number: (391) 11.02.01. September 1, 2013. Accessed May 10, 2014.
- Plagiocephaly and brachycephaly in the first two years of life: a prospective cohort study, Hutchison BL, Hutchison LA, Thompson JM, Mitchell EA. Pediatrics. 2004 Oct;114(4):970-80.
- Outcome Analysis of Cranial Molding Therapy in Nonsynostotic Plagiocephaly, Han-Su Yoo, Dong Kyun Rah, Yong Oock Kim. Arch Plast Surg. 2012 Jul; 39(4): 338–344. Published online 2012 Jul 13. doi: 10.5999/aps.2012.39.4.338. Full text
- Prevalence, risk factors, and natural history of positional plagiocephaly: a systematic review, Bialocerkowski AE, Vladusic SL, Wei Ng C. Dev Med Child Neurol. 2008 Aug;50(8):577-86. doi: 10.1111/j.1469-8749.2008.03029.x. Review. Full text
- Anthropometric Facial Proportions in Medicine, Edited by Leslie G. Farkas and Ian R. Munro, 344 pp, Charles C Thomas, Springfield, Illinois, 1987
- Positional plagiocephaly, part 1: a practical guide to evaluation. Consultant for Pediatricians. Taub PJ, Pierce P. December 20, 2010. Accessed March 1, 2014.
- Deformational brachycephaly in supine-sleeping infants, Graham JM Jr, Kreutzman J, Earl D, Halberg A, Samayoa C, Guo X. J Pediatr. 2005 Feb;146(2):253-7.
- Analysis of posterior plagiocephaly: deformational versus synostotic, Mulliken JB, Vander Woude DL, Hansen M, LaBrie RA, Scott RM. Plast Reconstr Surg. 1999 Feb;103(2):371-80.
- Plagiocephaly and craniosynostosis treatment. UnitedHealthCare. Medical Policy Number: 2013T0031K. November 1, 2013. Accessed May 30, 2014.
- International Classification of Diseases (ICD). World Health Organization. Accessed May 30, 2014.
- Head shape measurement standards and cranial orthoses in the treatment of infants with deformational plagiocephaly, McGarry A, Dixon MT, Greig RJ, Hamilton DR, Sexton S, Smart H. Dev Med Child Neurol. 2008 Aug;50(8):568-76. doi: 10.1111/j.1469-8749.2008.03017.x. Review. Full text
- Clinical classification of positional plagiocephaly, Argenta L, David L, Thompson J. J Craniofac Surg. 2004 May;15(3):368-72. Erratum in: J Craniofac Surg. 2004 Jul;15(4):705.
- The presentation of deformational plagiocephaly. Hylton-Plank L. Children’s Healthcare of Atlanta. JPO. 2004;16:S28-S30. Accessed June 9, 2014.
- Risk factors for deformational plagiocephaly at birth and at 7 weeks of age: a prospective cohort study, van Vlimmeren LA, van der Graaf Y, Boere-Boonekamp MM, L’Hoir MP, Helders PJ, Engelbert RH. Pediatrics. 2007 Feb;119(2):e408-18.
- Tummy Time Tools. Coulter-O’Berry C, Lima D. Children’s Healthcare of Atlanta and Orthomerica Products Inc. Accessed June 5, 2014.
- Prevention of deformational plagiocephaly in neonates, Cavalier A, Picot MC, Artiaga C, Mazurier E, Amilhau MO, Froye E, Captier G, Picaud JC. Early Hum Dev. 2011 Aug;87(8):537-43. doi: 10.1016/j.earlhumdev.2011.04.007. Epub 2011 Jun 12.
- Improving the lives of young children; increasing referrals and follow-up treatment in Medicaid and CHIP. Pelletier JE, Kenney GM. Urban Institute. Brief 2. Copyright © 2010. Assessed May 30, 2014.
- Neurological devices; classification of cranial orthoses-FDA. US Food and Drug Administration. US Code of Federal Regulations, Title 21, Volume 8, Revised April 1, 2012, CITE: 21CFR882.5970 Cranial Orthosis. Final rule. Fed Regist. 1998;40650-40652. Accessed March 1, 2014.
- Medicare coverage database. Centers for Medicare and Medicaid Services. Accessed May 10, 2014
| Further reading |
Identifying the Misshapen Head: Craniosynostosis and Related Disorders, Dias MS, Samson T, Rizk EB, Governale LS, Richtsmeier JT; SECTION ON NEUROLOGIC SURGERY, SECTION ON PLASTIC AND RECONSTRUCTIVE SURGERY. Pediatrics. 2020 Sep;146(3):e2020015511. doi: 10.1542/peds.2020-015511.
Nonsynostotic plagiocephaly: a child health care intervention in Skaraborg, Sweden, Lennartsson F, Nordin P. BMC Pediatr. 2019 Feb 6;19(1):48. doi: 10.1186/s12887-019-1405-y. Full text
Accuracy of measurements used to quantify cranial asymmetry in deformational plagiocephaly, Aarnivala H, Vuollo V, Heikkinen T, Harila V, Holmström L, Pirttiniemi P, Valkama AM. J Craniomaxillofac Surg. 2017 Aug;45(8):1349-1356. doi: 10.1016/j.jcms.2017.05.014. Epub 2017 May 22.
The course of positional cranial deformation from 3 to 12 months of age and associated risk factors: a follow-up with 3D imaging, Aarnivala H, Vuollo V, Harila V, Heikkinen T, Pirttiniemi P, Holmström L, Valkama AM. Eur J Pediatr. 2016 Dec;175(12):1893-1903. Epub 2016 Sep 13.
Analyzing infant head flatness and asymmetry using kernel density estimation of directional surface data from a craniofacial 3D model, Vuollo V, Holmström L, Aarnivala H, Harila V, Heikkinen T, Pirttiniemi P, Valkama AM. Stat Med. 2016 Nov 20;35(26):4891-4904. doi: 10.1002/sim.7032. Epub 2016 Jul 6.
Analysis of posterior plagiocephaly: deformational versus synostotic, Mulliken JB, Vander Woude DL, Hansen M, LaBrie RA, Scott RM. Plast Reconstr Surg. 1999 Feb;103(2):371-80. doi: 10.1097/00006534-199902000-00003.
Also see
Misshapen heads in infants create complicated assessment Contemporary Pediatrics
Newborn positioning, plagiocephaly screening, and parent education American Nurse today