
Can exercise prevent knee osteoarthritis?
A study of human skeletons housed in the vaults of US museums is providing a unique historical perspective on the prevailing wisdom that knee osteoarthritis (OA) is primarily a disease of aging and overweight, factors that are difficult if not impossible to prevent at the population level.

Skeletal knee joint with evidence of osteoarthritis. Ian Wallace
Jennifer Abbasi, JAMA November 22, 2017
In the recent comparison of bones from different periods, people born in the postindustrial era were substantially more likely to have knee OA than those born earlier, confirming a widespread belief that the condition is becoming more common.
More surprisingly, however, the increase in prevalence remained even after researchers controlled for risk factors including age and body mass index (BMI). The findings suggest that the commonly accepted risk factors may be incomplete.
“At a given age, if you were born after World War II you are more than twice as likely to have OA in your knee than if you had been born earlier, regardless of your weight,” said study co-author Daniel Lieberman, PhD, chair of the department of evolutionary biology at Harvard University.
Although the study, published in the Proceedings of the National Academy of Sciences, was not designed to identify factors driving up cases of knee OA, experts including those not involved with the research speculate that changes in physical activity may be an explanation.
| A Missing Link |
Lieberman decided to study osteoarthritis of the knee while writing a book on what he calls “mismatch diseases.” These conditions, like heart disease and diabetes, are more common or severe today “because our bodies are inadequately or imperfectly adapted to modern environmental conditions,” he explained.
While compiling a table of major mismatch diseases for the book, he had a realization: Although numerous epidemiological studies have indicated that knee OA is highly prevalent today, and that older age and obesity are strong risk factors, whether the disease’s prevalence can be explained by an ever-aging population and increasing obesity has never been tested.
“Because people are, on average, living longer today than they were a century or so ago, and because obesity has only become a public health crisis within the past few decades, many clinicians assume that knee OA is highly prevalent today because people are living longer and are more commonly obese,” said Ian J. Wallace, PhD, a postdoctoral researcher in Lieberman’s laboratory and first author of the new study. “Because there is an assumption that these are the risk factors that best explain the current prevalence of the disease, little attention is paid to prevention since aging is unavoidable and the obesity epidemic has been extremely difficult to tackle.”
To investigate these assumptions about risk factors, Wallace and academic collaborators documented cases of knee OA in more than 2000 skeletal remains of people who died between 1905 and 1940 during the early industrial era and between 1976 and 2015 during the modern postindustrial era. They also examined 176 skeletons from prehistoric hunter-gatherers and early farmers who lived between 6000 to 300 BP (before present, or years prior to 1950). To diagnose knee OA in cadaver collections from around the country, they looked for knee eburnation, a bone-on-bone polishing of the femur, tibia, and patella that occurs when cartilage is worn down in the late stages of degenerative joint disease.
All of the study subjects were at least 50 years old when they died, based on death records or age-related changes on the surface of their hip bones, and BMI was available from death records for most early industrial (84%) and postindustrial (64%) samples.
Knee OA has previously been documented in human fossils, and the new research confirmed that it’s an ancient ailment: 8% of prehistoric individuals in the study had the condition. It also appears to have become more common over the past century. Prevalence was 16% among the 819 postindustrial samples but only 6% in the 1581 early industrial samples.
On average, postindustrial individuals in the study were older and heavier when they died than preindustrial individuals, and age and BMI were positively associated with knee OA in these groups. But even after controlling for age and BMI, as well as sex and ethnicity, prevalence was still 2.1 times higher for people who died between 1976 and 2015 than for those who died between 1905 and 1940.
“I think that we all have in the back of our minds that it’s not just aging and obesity that is causing the increase in arthritis,” said Brian M. Grawe, MD, an orthopedic surgeon and assistant professor of sports medicine at the University of Cincinnati Academic Health Center, who was not involved with the work. “They basically proved that there is a missing link.”
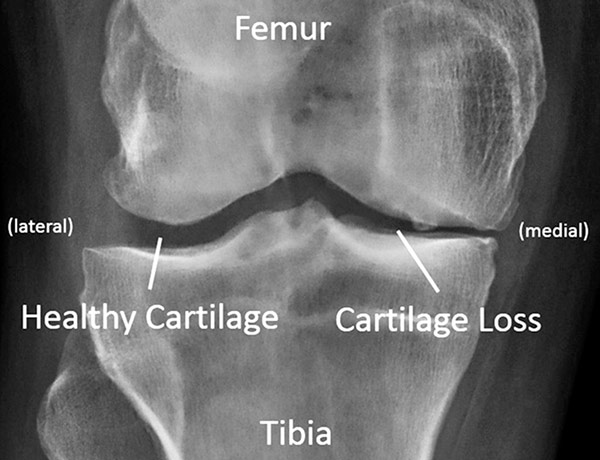
Figure 2: Standing knee x-ray for an individual with medial compartment knee osteoarthritis. The loss of articular cartilage is evident in the narrower gap in the medial compartment. Pete B. Shull PhD, Lower Extremity Review
| The Fitness Factor |
For now, the researchers can only speculate on what that missing link—or, more likely, links—could be. Experts agree that knee OA is almost certainly multifactorial, and Lieberman and his coauthors suggest plausible modern-day contributors ranging from inflammatory diets to hard pavements to the advent of footwear.
At the top of their suspect list is the shift toward more sedentary lifestyles. Research suggests that exercise can help prevent knee OA. According to David Felson, MD, a coauthor on the new study, physical activity within a certain range likely promotes the growth and maintenance of knee cartilage, ligaments, and bones, and strengthens muscles to appropriately distribute loads across the joint.
Felson is a professor of medicine and epidemiology at Boston University School of Medicine, where his research focuses in part on causes of osteoarthritis. “The absence of activity, the sort of sedentary lifestyles many of us have fallen into, may not be so healthy for our joints,” he said. “I think it’s a reasonable idea.”
Jeffrey Geller, MD, chief of the division of hip and knee reconstruction at Columbia University Medical Center, points to the fact that knee cartilage in adults has no blood supply other than that promoted by physical activity.
“Activity and weight-bearing forces the nutrients in the joint fluid to diffuse into knee cartilage, and that is its main source of nutrition,” he said. “There’s no formal mechanism other than the sort of pumping action of the mechanics of the knee.”
On the other end of the spectrum, physical activity-related knee injuries, like anterior cruciate ligament and meniscal tears, are a well-established precursor to knee OA, and could also be contributing to the increase in prevalence.
“That’s always been there and I’m sure that explains why some of the fossils we see that have OA got OA,” Lieberman said. But, he added, “people might be more susceptible to injury today because they’re weaker or they do more abnormal things, like skiing. We did not evolve to ski, I can tell you that as an evolutionary biologist.”
Although Felson agrees that sports factor into knee OA, “probably only about 10% of knee OA in older adults is related to recognized sports injuries from earlier in life. It’s not as big a factor as you might think,” he said.
But the extreme fitness trend of the past decade or so could create more knee OA cases—and knee replacements—down the line. “Things like CrossFit… I see people injuring themselves all the time that have no business doing these activities,” Grawe said. “It’s leading to a lot of injuries of the knee and ultimately it can lead to arthritis.”
There are already around 700 ,000 knee replacements every year in the United States, Geller said, and orthopedic surgeons estimate there may be a need for more than 2 million per year by 2025, potentially outpacing the supply of knee surgeons. Most of the increase will come from the growing aging population, according to Geller, but some may be related to other factors, such as obesity or physical activity levels.
Geller advises joint-friendly exercises. “Things like a stationary bike or an elliptical… are probably the best form of exercise because the impact on a joint is minimal,” he said.
Lieberman’s team is now looking at prevalence of knee OA in living populations from different parts of the world who have different lifestyles and levels of physical activity. Because physical activity and overweight influence each other, the researchers will try to control for both variables independently in these studies to parse their individual contributions to knee OA. The researchers are also focusing on the effects of physical activity on joints in general and cartilage in particular using animal models in the laboratory.
In the end, having a happy medium of physical activity may turn out to be a reasonable approach to warding off knee OA, along with maintaining a healthful diet and weight to reduce joint-damaging inflammation and abnormal load bearing.
“To me, what’s important about the paper is that it suggests that OA is much more preventable than we often assume,” Lieberman said.
Source Journal of the American Medical Association, JAMA
| References |
Knee osteoarthritis has doubled in prevalence since the mid-20th century, Wallace IJ, Worthington S, Felson DT, Jurmain RD, Wren KT, Maijanen H, Woods RJ, Lieberman DE. Proc Natl Acad Sci USA. 2017 Aug 29;114(35):9332-9336. doi: 10.1073/pnas.1703856114. Epub 2017 Aug 14. PDF
| Further reading |
Exercise as medicine to be prescribed in osteoarthritis, Ravalli S, Castrogiovanni P, Musumeci G. World J Orthop. 2019 Jul 18;10(7):262-267. doi: 10.5312/wjo.v10.i7.262. eCollection 2019 Jul 18. Review. Full text
Osteoarthritis: Trauma vs Disease, Jiménez G, Cobo-Molinos J, Antich C, López-Ruiz E. Adv Exp Med Biol. 2018;1059:63-83. doi: 10.1007/978-3-319-76735-2_3. Review.
Can Exercise Prevent Knee Osteoarthritis? Jennifer Abbasi. JAMA. 2017;318(22):2169–2171. doi:10.1001/jama.2017.16144
Muscle Power Is an Independent Determinant of Pain and Quality of Life in Knee Osteoarthritis, Reid KF, Price LL, Harvey WF, Driban JB, Hau C, Fielding RA, Wang C. Arthritis Rheumatol. 2015 Dec;67(12):3166-73. doi: 10.1002/art.39336.
The history of osteoarthritis-osteoarthrosis, J Dequeker, F P Luyten. Annals of the Rheumatic Diseases 2008;67:5-10. doi: 10.1136/ard.2007.079764
Also see
Health in a postindustrial age: The mystery of our creaky, painful knees
Skeletons say arthritis isn’t about aging — it’s about activity Quirks & Quarks, CBC Radio